Dr. Vikas Singh is a highly distinguished Consultant Urologist and Kidney Transplant Surgeon in Indore, recognized as one of the youngest surgeons in India to achieve the milestone of 100 individual kidney transplants early in his career. With a cumulative experience of over 500 kidney transplant procedures across premier institutions like PGI Chandigarh, Max Super-Speciality Hospital New Delhi, and SMS Medical College Jaipur, he brings world-class expertise to Central India. Now practicing at Kokilaben Dhirubhai Ambani Hospital Indore, Dr. Singh specializes in both conventional and cutting-edge Robotic-Assisted Kidney Transplant surgery—a minimally invasive approach that offers patients faster recovery, reduced pain, and excellent graft outcomes. His comprehensive transplant program manages the entire journey from pre-transplant evaluation and donor workup to post-operative care and lifelong follow-up, ensuring the highest success rates and quality of life for transplant recipients. We provide complete transparency regarding treatment costs and facilitate seamless coordination with insurance providers and government schemes for our patients throughout Central India.
Consultant Surgeon at Kokilaben Dhirubhai Ambani Hospital, Indore, equipped with advanced laser and endoscopic technology.
Extensive expertise in managing simple to complex urethral strictures with hundreds of successful procedures.
Proficiency in both minimally invasive (OIU/Laser) and definitive open reconstruction (urethroplasty) techniques.
Urethral stricture is an abnormal narrowing of the urethra (the tube carrying urine from bladder to outside) caused by scar tissue formation. This narrowing restricts urine flow, leading to bothersome symptoms and potential complications if untreated. Strictures can occur anywhere along the urethra but are most common in the bulbar (mid) and anterior portions.
The most frequent causes include traumatic catheterization (prolonged or difficult catheter insertion), previous urethral instrumentation or surgery, pelvic trauma or straddle injuries, infections (especially untreated STIs), lichen sclerosus (skin condition affecting the urethra), and congenital abnormalities. In many cases, no specific cause is identified (idiopathic strictures).
Classic symptoms include weak urinary stream, straining to urinate, sensation of incomplete bladder emptying, urinary frequency and urgency, recurrent urinary tract infections, post-void dribbling, and in severe cases, complete urinary retention (inability to pass urine). These symptoms progressively worsen over time and significantly impact quality of life.
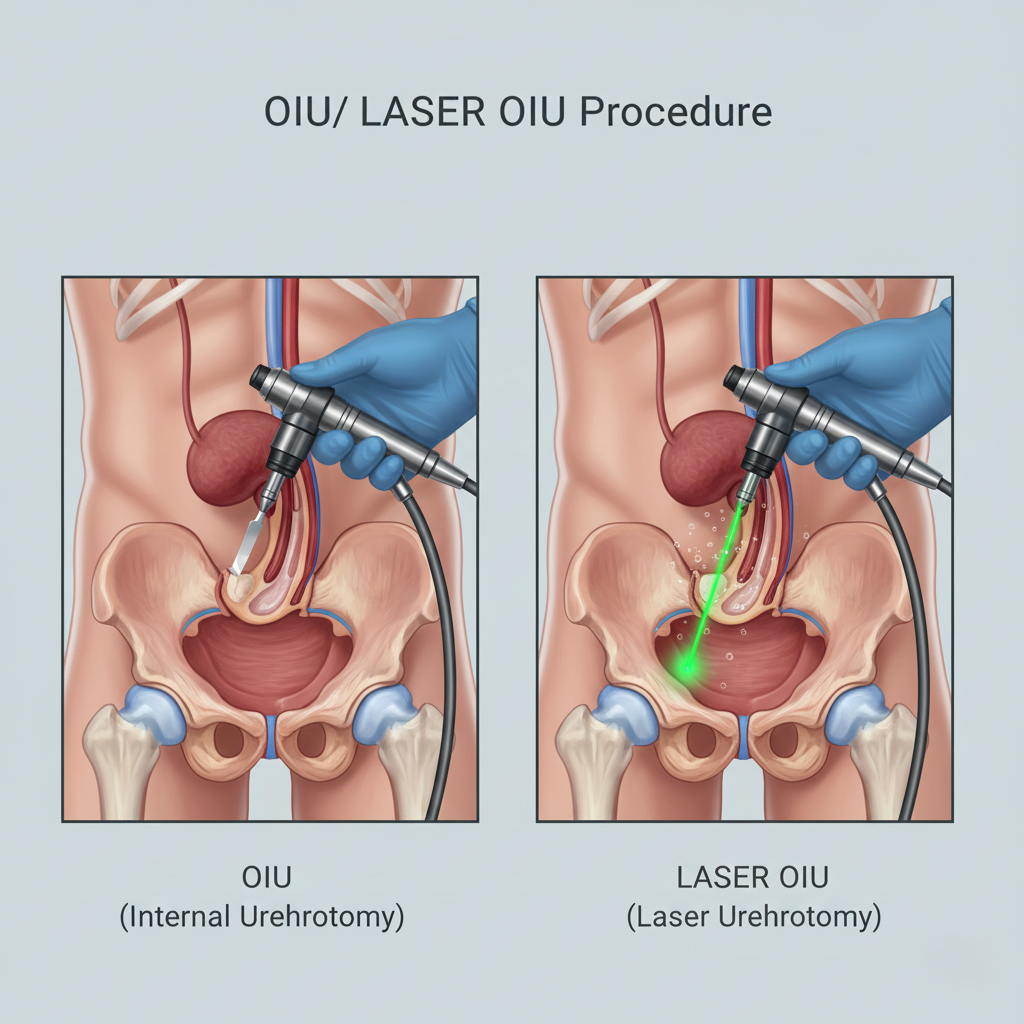
OIU is a minimally invasive endoscopic procedure where a small knife (cold knife or electrocautery) is passed through a scope to make precise incisions in the stricture, opening the narrowed segment. Performed under anesthesia through the urethra with no external incision, it’s effective for short, simple strictures (<1.5 cm). A catheter remains for 3-7 days post-procedure. Recovery is quick (few days), but recurrence rates are 40-60% for first-time procedures, higher with repeated OIUs. Best For: First-time treatment of short, simple strictures; quick symptom relief with minimal invasiveness.
Laser OIU represents the modern evolution of traditional OIU, using high-precision Thulium Fiber Laser or Holmium laser to incise strictures with exceptional accuracy. The laser’s bloodless cutting ability allows better visualization, more precise depth control, and reduced scar tissue formation compared to cold knife or cautery. The procedure is similarly performed endoscopically with catheterization for 3-7 days. Laser OIU may have slightly lower recurrence rates (35-50%) due to more controlled tissue handling. Best For: Short to moderate strictures where precision and minimal bleeding are advantageous; preferred modern approach over conventional OIU.
For recurrent strictures, long strictures (>1.5-2 cm), or complex cases, urethroplasty is the gold standard offering definitive cure. This open surgical reconstruction involves removing the scarred segment and either reconnecting healthy ends (anastomotic urethroplasty) or using grafts/flaps (tissue from inside cheek or skin) to widen the urethra. Though more invasive with longer recovery (3-4 weeks), success rates exceed 85-95% with minimal recurrence—a true cure rather than temporary fix. Best For: Recurrent strictures, long strictures, complex cases; patients seeking definitive one-time solution.
Diagnosis is confirmed through uroflowmetry (measuring urine flow rate), retrograde urethrography (X-ray imaging of urethra), and sometimes cystourethroscopy (direct visualization). These tests determine stricture location, length, and severity, helping Dr. Singh select the optimal treatment approach.
Performed under spinal or general anesthesia, the procedure takes 20-40 minutes. A specialized endoscope is passed through the urethra to visualize the stricture. Using either a small blade (conventional OIU) or laser fiber (Laser OIU), Dr. Singh makes 1-3 precise radial incisions through the scar tissue at the 12 o'clock position, immediately opening the narrowed segment and restoring urethral caliber.
A urinary catheter is placed for 3-7 days to keep the urethra open while healing occurs. This allows the incised tissue to heal in an expanded position rather than scarring down again. Some surgeons inject steroids or mitomycin to reduce recurrence risk. The catheter is removed in the office, and most patients urinate normally immediately afterward.
No external incisions or visible scars entire procedure performed through natural opening (urethra).
Most patients return to normal activities within 3-5 days after catheter removal; minimal discomfort.
Typically performed as day-surgery with discharge the same day or next morning; no extended hospitalization.
Dramatic improvement in urinary stream noticed immediately after catheter removal in successful cases.
Schedule a private, confidential consultation with Dr. Singh in Indore.
The treatment choice depends primarily on stricture characteristics and treatment history. For first-time, short strictures (<1.5 cm) in accessible locations, OIU or Laser OIU is typically recommended as the initial approach—it’s minimally invasive with quick recovery and reasonable success rates (40-60%). Laser OIU may be preferred for its precision and reduced bleeding. However, if you’ve already had one or more failed OIUs, have a long stricture (>2 cm), or have a complex stricture involving difficult locations, urethroplasty becomes the better choice despite being more invasive, as it offers definitive cure (85-95% success) rather than repeated temporary fixes. Dr. Singh will evaluate your specific situation through imaging studies and recommend the approach offering the best long-term outcome for your particular stricture.
Success rates for OIU/Laser OIU depend significantly on stricture characteristics and whether it’s a first treatment or repeat procedure. For first-time OIU on ideal candidates (short, soft, single strictures), success rates are approximately 50-60%, meaning about half of patients achieve durable relief. However, success rates decrease substantially with repeated procedures—second OIU succeeds in only 30-40%, and third or subsequent OIUs have even lower success. Recurrence typically occurs within 3-12 months if it’s going to happen. Factors predicting better success include shorter stricture length (<1 cm), bulbar location, traumatic rather than inflammatory cause, and first-time treatment. If a stricture recurs after 1-2 OIUs, continuing with repeated endoscopic treatments often leads to increasing scar tissue formation, making eventual urethroplasty more challenging—this is why Dr. Singh carefully counsels patients on realistic expectations and the appropriate time to consider definitive reconstruction.
Laser OIU offers several technical advantages over traditional cold-knife urethrotomy. The Thulium Fiber Laser or Holmium laser provides virtually bloodless incision, allowing superior visualization throughout the procedure—blood obscuring the view is a common problem with cold-knife techniques. The laser’s precision enables more controlled depth of incision, reducing risk of cutting too deep (causing bleeding or perforation) or too shallow (inadequate stricture opening). The thermal effect of laser may cause less immediate inflammation and potentially reduces aggressive scar reformation, though recurrence rates remain similar. The hemostatic properties make it safer for patients on blood thinners. From a patient perspective, the procedures are similar in terms of recovery and outcomes, but the technical refinements may translate to slightly better success rates and reduced complications in experienced hands. Dr. Singh utilizes laser technology when available as it represents the modern standard of endoscopic stricture management.
The urinary catheter typically remains in place for 3-7 days after OIU/Laser OIU, though duration varies based on stricture severity and surgeon preference. The catheter serves two purposes: allowing the incised urethra to heal in an open position and preventing early re-scarring. During this period, you’ll have a drainage bag attached—smaller leg bags can be worn discreetly under clothing during the day, with larger bedside bags at night. Catheter care involves keeping the insertion site clean, ensuring the tube doesn’t kink or pull, drinking adequate fluids, and emptying the bag regularly. Bladder spasms (sudden urge to urinate despite catheter) are common and managed with anticholinergic medications. Most patients manage catheters at home comfortably with proper instruction. Catheter removal is a simple office procedure taking seconds—most patients urinate normally immediately afterward if the procedure was successful.
While there’s no guaranteed way to prevent recurrence, several strategies may reduce risk. After OIU/Laser OIU, some urologists use adjuvant therapies like steroid injections or mitomycin application to the incision site, which may modestly reduce recurrence by limiting excessive scar formation—though evidence is mixed. Self-catheterization (periodically passing a catheter yourself at home) is sometimes recommended to keep the urethra dilated, but compliance is difficult and effectiveness uncertain. The most important factors are treating underlying causes (managing lichen sclerosus if present, avoiding traumatic catheterizations, treating infections promptly) and realistic treatment selection—knowing when to proceed to definitive urethroplasty rather than repeated failed OIUs that worsen scarring. For patients with recurrent strictures after 1-2 endoscopic treatments, Dr. Singh typically recommends definitive reconstruction rather than endless cycles of temporary procedures, as urethroplasty offers genuine cure in most cases.
Most patients experience no adverse effects on sexual function after OIU or Laser OIU. The procedure is performed in the urethra and doesn’t involve structures responsible for erection (cavernosal nerves and blood vessels) or ejaculation (ejaculatory ducts and seminal vesicles). However, temporary restrictions apply—sexual activity should be avoided for 2-3 weeks after catheter removal to allow complete healing. Some patients report temporary changes in ejaculation or mild discomfort during initial sexual activity, but these typically resolve within 4-6 weeks. It’s important to note that if a stricture eventually requires complex urethroplasty (especially for very long strictures requiring extensive grafting), there may be slightly higher risks to sexual function, but simple endoscopic procedures like OIU have minimal impact. Any concerns about sexual function should be discussed with Dr. Singh before treatment, as preserving these functions is always a priority in treatment planning.
The leading center for advanced, compassionate urological care and treatment in Indore, Madhya Pradesh.
