
Kidney Transplant is a surgical procedure that’s a second chance at life for people at end-stage kidney failure. Once the surgery is completed, there are many things that people are able to do such as unrestricted eating, travel without worry, sleep through the nights and not have to do dialysis and most importantly, feel like yourself.
Dr. Vikas Singh is a Senior Consultant Urologist and Kidney Transplant Surgeon at Kokilaben Dhirubhai Ambani Hospital, Nipania, Indore and is a certified world-class transplant surgeon from Central India. He is the youngest surgeon in India to have completed a milestone 100 kidney transplant surgeries. He also has participated in over 500 kidney transplants across the country in premier institutes like PGI Chandigarh, Max Super-Speciality Hospital New Delhi, and SMS Medical College Jaipur.
It is a matter of great pride for the people of Madhya Pradesh, and Chhattisgarh and surrounding Areas. Indore is now home to one of the finest kidney transplant services that is available in Delhi or Mumbai.
Kidneys are located just below the ribs on the spine and are responsible for filtering blood and other important functions in the body. They also help regulate blood pressure and maintain balance of important minerals in the body. They filter blood and in the process create urine. On an average day the kidneys filter about 200 liters of blood.
Due to the importance of the kidneys and their filtering functions, many diseases can cause the kidneys to be damaged to the point where they can no longer do their jobs. This is called End-Stage Renal Disease (ESRD) or kidney failure. Once kidneys enter this stage the only options left are intensive and add in continued support for the kidneys (dialysis) or to replace the damaged kidneys with donor kidneys (kidney transplant)
During a kidney transplant the damaged kidneys are removed and a healthy kidney (from a living or deceased donor) is surgically placed in the donor’s lower abdomen. This is done through a series of vascular and urological anastomoses.
Most of the time, in a transplant, the patient\textquotesingle s own failed kidneys are not removed. The transplanted kidney just takes on the work the failed kidneys cannot do. With the right care and medication, a transplanted kidney can function for 15-20 years if transplanted from a living donor, or 10-15 years if transplanted from a deceased donor.
Patients with End-Stage Renal Disease (ESRD) are recommended for a kidney transplant. This is the final and irreversible stage of chronic kidney disease (CKD) where kidneys function <10-15% of their capacity. At this point, the body can no longer sustain itself without either renal dialysis or a kidney transplant.
In India, common causes of End Stage Renal Disease (ESRD) include:
If you or a family member are on dialysis or have kidney function less than 15%, you need to speak with Dr.
Vikas Singh regarding whether kidney transplants are an option for you.
Kidney transplants can be classified based on transplant type, and the type of donor organ and its relationship to the recipient among many factors, and summarised as follows:
Transplants from living donors is the gold standard in cases of suitable donors, and in a transplant of this type, a living, healthy, and injury-free donor, usually a relative, donates one of their two healthy kidneys, and living donation is usually very safe for the donor, since one can live perfectly healthy and normal with one healthy kidney.
A transplant from a living donor has many benefits. First, the transplant can be asndcheduled at an agreed-upon time, as opposed to waiting for an available organ. Secondly, living donor kidneys have better longevity of an average of over 15 to 20 years than kidneys from deceased donors. Also, the recipient’s body is usually better prepared, since often, better pre operative evaluation can be done, due to the planned organ donation.
At Kokilaben Hospital, living donor nephrectomy, that is, surgery to remove the donor’s kidney, is done laparoscopically by Dr. Vikas Singh, which is a type a surgery that uses small incisions like a keyhole and avoids an open large cut. This type of surgery facilitates less pain and blood loss, and reduces the time to recover. Because of this, the donor usually goes home after 2-3 days, and 3-4 weeks is normal activity.
A deceased donor transplant uses a kidney from a donor who has been declared brain dead – where the brain has permanently and irreversibly stopped functioning, and the heart can still be beating under ventilator support. It involves a generous act of organ donation by the family of the brain dead person, which gives the transplant recipient as chance at life.
In India, organ transplant from deceased donors are facilitated through the government mandated organ sharing system. Patients receiving kidney transplants from deceased donors are put on a waiting list and matched to a donor based on blood group, waiting time and other medical criteria. Due to limited supply of deceased donor organs in India, it results in prolonged waiting periods and many patients await for transplants for extended periods of time.
Compared to living donor kidneys, deceased donor kidneys have shorter average graft survival of about 10 to 15 years, but remain a life transforming treatment as they are far better than being on dialysis. Kokilaben Dhirubhai Ambani Hospital is a registered transplant center and has been a participant in the deceased donor organ sharing system.
Indian law under the Transplantation of Human Organs and Tissues Act (THOTA) separates living donors into two broad categories: near relatives and unrelated donors:
It is not as simple as stating every patient with kidney failure can receive a transplant, and every willing donor can provide a donation. Preparatory medical assessments on both sides, recipient, and donor, are crucial components of planning kidney transplant surgery.
Medical Criteria for Recipients
For the most part, there are no other requirements aside from the following for one to be eligible for a kidney transplant:
Patients are not ruled out completely in the presence of controlled cardiovascular disease, diabetes, and obesity, but these conditions will make the patient a higher risk. These conditions are assessed individually and one can expect that a nephrologist and other specialists in transplant surgery will work together in eliminating or improving the medical condition before a surgery is offered.
Patients are not completely ruled out by being elderly as there is no upper age limit. Many patients in their 60’s and 70’s can and have received successful transplants. Each case is assessed to determine the patients overall health and biological fitness.
Medical Criteria for Donors
Living kidney donors are all required to go through rounds of extensive evaluations to assess that it is a safe procedure for them and that the kidney will be able to perform adequately in the new host. Some of the criteria include the following:
Assessments for donors consist of blood and urine examinations, CT angiography (which evaluates both the kidneys and blood vessels), cardiac assessments, and psychological evaluations. Donors are only cleared for surgery after all tests affirm that donation would be safe.
Kidney Transplant Steps
Kidney Transplantation is a planned procedure and is carried out in multiple stages. Knowledge of the steps in the process provides the patient and their attendants a sense of preparedness and helps manage expectations.
Before surgery is scheduled, both recipient and donor must first complete a working up process at Kokilaben Hospital, beginning with:
In order for the donor to complete all the above tests, they must undergo a CT angiogram of the kidneys to assess kidney anatomy and blood supply to determine the safest and MOST optimal kidney for donation.
Of significant consideration, aside from the crossmatch test, are the following:
In some instances, blood group incompatible or crossmatch barriers can be addressed by the use of a desensitisation protocol involving plasmapheresis and immunomodulation. This is done at a specialized transplant centre and requires a lot of planning.
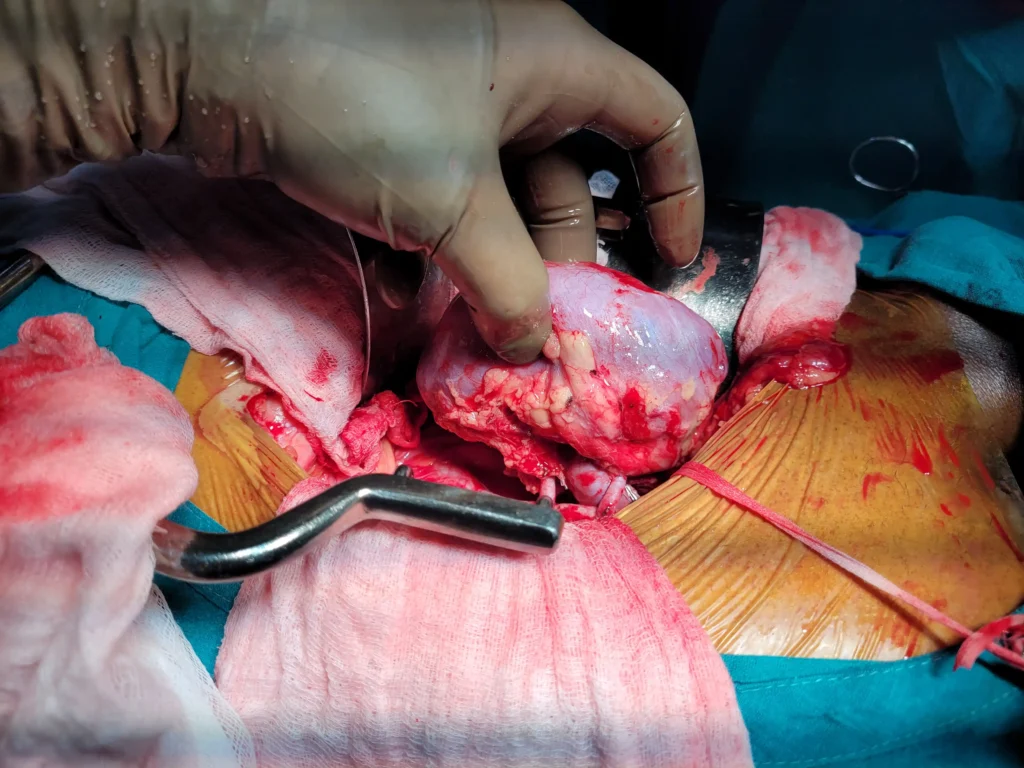
Surgery to implant a kidney takes 3-4 hours and is done while a patient is under general anesthesia. Here is a brief overview of the process:
After making the incision in the lower abdominal region, usually on either the right or left side, Dr. Vikas Singh skillfully positions the donor kidney in the lower abdomen/pelvic region. This region allows for easy access of the blood vessels and bladder.
The urine carrying tube (ureter) of the donor kidney is connected to the recipients bladder. Then, the donor kidney’s blood vessels (renal artery and renal vein) are joined to the patient’s iliac artery and vein (large blood vessels of the pelvis) so blood supply is reestablished to the new kidney.
When blood supply is returned to the new kidney, it is a great sign of a functioning transplant, and it will often produce urine right away. In some, especially those who receive a kidney from a deceased donor, the new kidney can take a while (days to weeks to even longer) before it produces urine, and dialysis will still be required during that interim.
After a urinary catheter is placed to drain urine from the bladder, a drain may be placed to the new kidney to collect fluid. Then, the patient goes to the recovery room and later to the post-transplant care unit. Here, the team will monitor the function of the new kidney along with blood pressure, fluid balance, and rejection symptoms.
Your remaining kidneys will be constantly evaluated from the first few days and weeks of your post-surgery-care. At Kokilaben Hospital, your kidneys will be monitored through daily blood (for urea and electrolytes) and urine tests. Immunosuppressive treatment will also begin, as you will need to start these medications to avoid your body rejecting the transplant.
Typically, transplant patients are discharged from the hospital after 5 to 10 days, assuming there are no complications and the transplant kidney is functioning well. After discharge, followed by regular visits. In the first month after transplant, visits may be every few days, and these will start to be spaced to monthly, quarterly, and eventually, as your kidney function stabilizes, these visits will not be needed.
Post transplant, you will take more than a few medications to help your body accept the transplant and avoid causing an attack. These medications are called immunosuppressive medications, and you will take them as long as the kidney transplant is functioning. A few of the bigger players in these medications are tacrolimus and prednisolone, and as the risk of an acute rejection decreases, the doctors will taper your dosages in time. Most of these drugs are started in higher dosages, and tapering is done to lower doses.
Post Kidney Transplant: Recovery & Follow-Up
Post transplant there is a major shift for your quality of life. After your transplant there is a sharp pivot away from use of your dialysis machine. While people describe the recovery after a transplant to be a miraculous period for of rejuvenated energy the post transplant period is as much about responsibility as it is about feeling better.
You will have to adopt your anti-rejection medications as a new daily ritual. Missing these medications has consequences. Worse case scenario is the your body rejecting the new kidney. So, believe it or not it is vital to take your anti-rejection medications every day. More than one transplant doctor will prescribe a trifecta of medicines. Most commonly, prednisolone, tacrolimus, and the infamous mmf (mycophenolate mofetil). It should be noted that these drugs do not have a set dosage for the duration of a patient’s life. These medicines will have their dosages altered over time. This is result of periodic tests that assess your kidney function and blood levels.
Visits to your transplant doctor will be frequent at the start. Ideally this will lessen over time. Doc Singh will adjust the lad and kidney function tests to custom calibrate your dosages. Initially you will spend a part of your weekly schedule at your doctor for weekly blood tests. Then as your new kidney stabilizes your visits will decrease to monthly, quarterly, and so on.
Diet and Lifestyle – After transplant, many of the restrictions on fluid and potassium intake from dialysis are lifted, and patients can enjoy an expanded selection of foods. To protect the heart and the new kidney, a heart-healthy diet is recommended. This includes plenty of vegetables and whole grains, and lean sources of protein. Some immunosuppressive regimens can cause weight gain and increase blood sugars. Patients are encouraged to maintain a healthy weight. Staying active is also strongly advised, along with avoiding smoking and alcohol consumption.
Infection Awareness – Because of the immunosuppressive regimens, patients are at an increased risk for infections. Patients should thorough and vigilant for signs of infection along with unexplained fevers and other strange symptoms. They should reach out to the transplant team with those concerns. Patients should get non-live vaccines, but live vaccines are typically avoided after a transplant.
Monitoring for Rejection – The first year after transplant is the highest risk period for Acute Rejection. Acute Rejection is an immune response to a transplanted kidney. Some common symptoms are increased creatinine levels, decreased urine output, swelling, and fever. The good news is that, if detected early, Acute Rejection is treatable with a short course of steroids and other medications.
Adjusting to a New Normal – After a transplant, most patients return to their daily activities and light work within four to six weeks. It typically takes four to six weeks to return to driving. For the first three months, patients are advised to avoid heavy lifting and strenuous activities. Women should consult their transplant team about their post-transplant medications, and how they may affect pregnancy, before becoming pregnant. It is advised to wait 1-2 years after transplant before trying.
Risks & Complications of Kidney Transplant – What You Should Know
Kidney transplant is major surgery, and like all major surgeries, there are associated risks. Dr. Vikas Singh believes in transparency. People should understand both the good and the bad before deciding.
Surgical Risks – As with any surgery that requires general anaesthesia, there are risks of bleeding, blood clots, infections in the wound, and complications related to the anaesthesia itself. Pre-operative assessments and the anaesthetists paired with surgeons at Kokilaben Hospital, help reduce these risks.
Delayed Graft Function (DGF) – Transplanted kidneys, especially with deceased donor kidneys, may take a long time to start functioning. Patients may continue to be on dialysis, but it is usually temporary. Most kidneys that are delayed do eventually start functioning.
Acute Rejection – This is the most important complication in the first year. The donor kidney is registered as a foreign object, and an immune response occurs. If this is caught in time, and it is treated with an adjustment to immunosuppression, there is usually no permanent damage to the kidney.
Chronic Rejection – Transplanted kidneys can fail due to chronic rejection. The kidneys are gradually and slowly damaged due to the immune system. The most effective way to combat this is taking medications as prescribed, and consistent follow up.
Infections: due to the nature of immunosuppressants, infection of some kind will occur post transplant. More common infection will be of the Broncho Pulmonary system (Pk). The use of body-sampling-antiviral medications are to cover the post transplant patient while they perform surgery and place the various body-sampling-antiviral medications.
Side Effects of the Medication: Most common infections due to the nature of the body-sampling-antiviral medications are bone thinning, risking fractures, skin, and various infections. Long-standing infections of the body can occur due to many various reasons.
If the transplanted kidney fails, due to prolonged infections, the patient can start with the dialysis process again. If the patient has multiple infections, they will be placed again, to wait on the transplant list.
Understanding which of the above infections do occur is worth it. For many without the transplant, there is a vast range of benefits, compared to the post transplant dialysis. The team at Kokilaben Hospital are with each patient and actively working with the various and best team, which can be aligned with the great level of East/West, while the level of the various medications are at the transplant patient level.
Why should you choose Dr. Vikas Singh for Kidney Transplants in Indore?
Surgeon selection is always going to be the most important choice to make to you and your family. This is why numerous families across central India have placed their trust in Dr. Vikas Singh.
Dr. Vikas Singh is India’s youngest surgeon to single handedly achieve the landmark of 100 Transplants. In addition, he has been a part of \5\00 other transplants across various institutions like \PG\I Chandigarh, Max Super Speciality \H\ospital New Delhi, \S\MS Medical College Jaipur. This type of experience is uncommon in major metros and is available at large volume transplant centers.
Dr. Vikas Singh has been a key surgeon in bringing the most modern kidney transplant surgery to numerous hospitals throughout Madhya Pradesh and other states in the republic. One of Dr. Vikas’s impressive attributes is that he made a personal commitment to make this life-saving surgery available to the population of India, specifically to central India, which exemplifies a great deal of his professional legacy.
Dr. Vikas Singh uses the laparoscopic (keyhole) technique for operating on the living kidney donors. This technique, is associated with a lower level of post operative surgical pain, less blood loss and significantly shorter recovery time when compared to open surgery. This makes the decision to become a living kidney donor, much less of a burden to the donating family member.
PGI Chandigarh, Max Hospital New Delhi, SMS Medical College Jaipur, Choithram Hospital Indore - Training by Dr. Vikas Singh is as good as it gets in Urology and transplant and more than just understanding the full complexities of renal transplant. He gets training in the full breadth and depth of high volume complexity.
Dr. Vikas Singh and his team manage every balance of the transplant continuum - from the first evaluation and donor workup, to the setting, and hospitalisation and followup, that spans years. Patients are not forgotten and dropped - they receive constant, persistent, seamless, integrated service, relatively to a team that is well acquainted with their case.
Kokilaben Dhirubhai Ambani Hospital, Nipania, Indore is outfitted with state of the art construction models of theatres, construction models of intensive care units, construction model of modern labs, and construction models of assorted team of nephrology, anaesthesia, and transplant coordination, construction models of everything required and more for the safe and successful performance of renal transplantation.
Posted onTrustindex verifies that the original source of the review is Google. Dr sahab badiya nature he or samjhate bhi bahut ache se haiPosted onTrustindex verifies that the original source of the review is Google. Dr Vikas Singh Urologist of KDAHOSPITAL is an excellent Doctor. During and after my Operation Dr Singh took personal care. Dr Singh supporting staff are very caring. I recommend patients suffering from UTI, Prostate Gland problems, Kidney Stone, etc to take treatment from Dr Vikas Singh (Retired Senior Professor Pradeep Kundal from Jhabua Madhya Pradesh)Posted onTrustindex verifies that the original source of the review is Google. Bhut achha sir hePosted onTrustindex verifies that the original source of the review is Google. Sir me Mera peostate ka operation kiya tha ab me puri tarah thik hu or mujhe urine bhi bahut ache ata hePosted onTrustindex verifies that the original source of the review is Google. Excellent doctor and great in naturePosted onTrustindex verifies that the original source of the review is Google. Good dr Vikas sirPosted onTrustindex verifies that the original source of the review is Google. 10 mm kidney stone removed via RIRS method, thank you very much Dr Vikas Sir.Posted onTrustindex verifies that the original source of the review is Google. Nice Dr for prostate treatment at kokilaben hospital.
Kidney lifespan for a living donor transplant is approximately 15-20 years. For a deceased donor transplant, kidneys last about 10-15 years. Certain measures may also allow for transplanted kidneys to last beyond these averages. Measures include excellent adherence to medication, a healthy lifestyle, and a consistent transplant clinic follow-up. In patients where a transplanted kidney fails, dialysis may be reinstated. An additional transplant is also a possibility.
Yes, living kidney donation is safe for the majority of donors. Humans have two kidneys, and being a donor means only having one. Healthy donor candidates report comparable life outlooks and living experiences to peers of the same age and health status, who have not donated a kidney. The donor surgery is performed by laparoscopy by Dr. Vikas Singh and is also less of a burden to the donor.
Typically, kidney recipient and donor blood group compatibility is required. In the case of a willing donor who is blood group incompatible, a swap (paired) transplant is an option, where two incompatible pairs of donors are exchanged so both recipients get a compatible kidney. In certain specialist centres, there are also ABO incompatible transplants with dessensitization. Dr. Vikas Singh will help determine the best option for you.
In India, the average wait time for a deceased donor kidney is highly state-dependent, and can vary based on the blood group, kidney demand, and organ supply. India has a disproportionately high demand for deceased donor kidneys, thus, living donor transplants, when possible, are highly encouraged as it eliminates the wait time.
In Indore, under the care of Dr. Vikas Singh, and at Kokilaben Dhirubhai Ambani Hospital, all forms of kidney transplants (both living and deceased donor) are available. It is no longer required for kidney transplant surgery to be travelled for patients from Madhya Pradesh and Central India to Delhi or Mumbai, we have world-class transplant care in Indore.
For experienced surgeons, India has a one year success rate of over 95% for transplants from living donors. Achieving a one year success rate for transplant surgeries from deceased donors is 85 to 90%. However, outcomes are greatly affected by the patient’s overall health and adherence to post-surgery medication. Dr. Vikas Singh’s team has outcomes that are consistent with these numbers.
Yes, the remaining kidney undergoes something called compensatory hypertrophy, where it increases its function to ~70-75% of what both kidneys provided. ThIs is more than enough for normal, healthy daily living. Most living kidney donors continue to live normal lives after the donation, without any significant, detrimental, long-term effects on their health.
Yes, there is no age limit for receiving a kidney transplant. Patients in their 60s, 70s, or older can receive a transplant, as long as the person is medically fit enough to receive the procedure. It is a decision based on the complete evaluation of the person’s health, cardiac health, and life expectancy, not strictly based on age. Dr. Vikas Singh treats older patients individually and do not dismiss patients simply because of age.
Post-transplant, patients are on a lifelong regimen of daily medications called immunosuppressive medications. For as long as the kidney is functioning, which is usually for life, patients are on these medications. These medications include tacrolimus, mycophenolate mofetil (MMF), and a low dose steroid. These are the main medications and specific dosages are adjusted at each follow up. These medications are what keep the kidney functioning, therefore, patients are at an increased risk of rejection and losing the kidney, if they stop the medications.
You may call the number or visit the address. All relevant medical reports will be required. This includes your kidney function reports, dialysis reports, and imaging like ultrasounds or CT scans, as well as your current medications. After the initial consultation and assessment, options will be outlined, and the next steps will be explained by Dr. Vikas Singh.
24/7 Services Available

Copyright © 2026 Urology Center | All Rights Reserved
Design and Developed by Namastetu Technologies Pvt.Ltd